
What’s Changing for RPM in 2026?
In July 2025, the Centers for Medicare & Medicaid Services (CMS) released its proposed 2026 Medicare Physician Fee Schedule (PFS) rule. Among the most significant updates are changes to the billing codes and requirements for Remote Patient Monitoring (RPM). These changes are designed to make RPM more accessible, flexible, and aligned with real-world clinical practice. Here’s everything you need to know.
Key Proposed Changes for 2026
1. RPM Device and Data Transmission: Ending the “16-Day Rule”
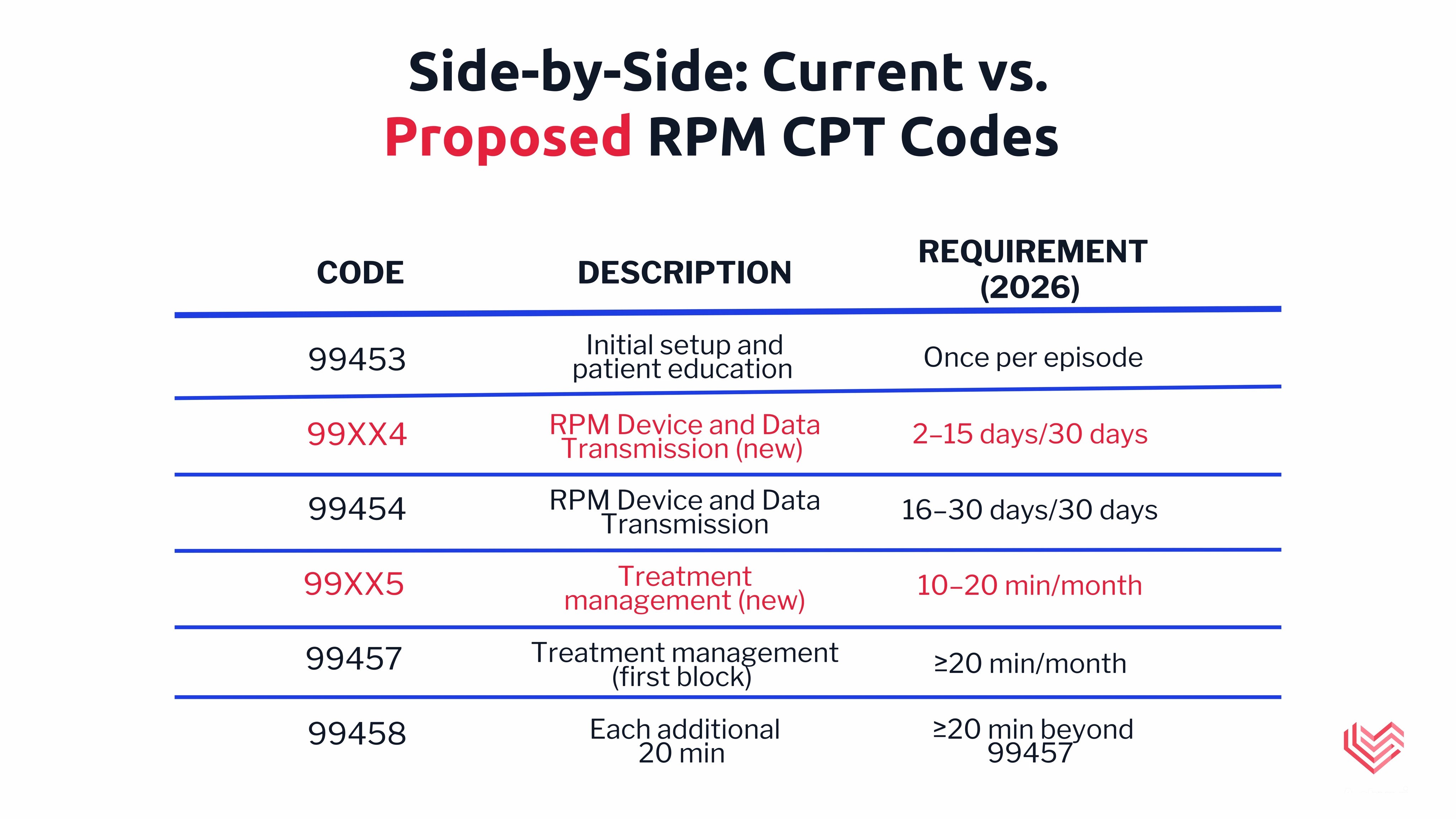
Current Rule: To bill for RPM device and data transmission (CPT 99454), providers must collect and transmit data for at least 16 days in a 30-day period.
Proposed Change:
New Code (99XX4): Allows billing for 2–15 days of RPM device and data transmission in a 30-day period
Revised 99454: Will now cover 16–30 days of RPM device and data transmission in a 30-day period.
Impact: Providers can bill for patients who need less frequent monitoring. For example, a patient recovering from surgery who only needs to be monitored twice a month, or a patient on a new medication who benefits from weekly blood pressure checks, would now qualify for RPM billing. This opens RPM to a broader patient population.
2. Treatment Management Codes: Lower Time Thresholds
Current Rule: CPT 99457 covers the first 20 minutes of clinical staff time per month; CPT 99458 covers each additional 20 minutes.
Proposed Change:
New Code (99XX5): Allows billing for 10–20 minutes of RPM management services, reimbursed at about half the rate of the 20-minute code.
99457 and 99458: Will keep their current 20-minute thresholds; CMS did not accept the AMA’s proposal to lower these to 11–20 and 10-minute increments.
Impact: Providers can now bill for shorter—but still meaningful—patient interactions. For example, a 12-minute phone call to review a patient’s blood pressure readings, discuss medication adherence, or respond to an alert from the monitoring device, would now be billable.
3. Reimbursement and Policy Notes
Reimbursement Stability and Review: The new codes are proposed to be reimbursed at rates similar to current codes, but CMS is using outpatient prospective payment system (OPPS) cost data rather than the previous practice expense relative value unit (PE RVU) method. This means reimbursement rates may change in the future as CMS collects more data and adjusts values, and rates for the new codes could be updated after further review. Providers should monitor CMS updates for finalized rates and any future adjustments. Federal Register – see official rule
Long-Term Focus: CMS emphasizes that RPM is a longitudinal (ongoing) service, not a short-term episode. RPM can continue as long as there is a documented medical need.
What These Changes Mean for Providers
Expanded Patient Access
The new 2–15 day billing option means RPM can be offered to patients who don’t require daily monitoring. This includes patients using GLP-1s for weight loss, those needing weekly weigh-ins, or postoperative patients needing only short-term oversight.
Increased Operational Efficiency
The new 10-minute management code ensures clinical staff are compensated for brief but important interactions. This eliminates the “wasted” time of a 15-minute call that previously went unbilled.
Financial Sustainability and Growth
With more billable options and stable reimbursement, practices can enroll more patients and scale RPM programs with greater confidence. For instance, clinics can now include patients who previously didn’t meet the 16-day threshold, supporting broader adoption of digital health.
Compliance and Documentation
Providers should continue to document medical necessity and patient engagement, as RPM remains a service for ongoing care rather than short-term episodes.
Frequently Asked Questions
When do these changes take effect?
If finalized, these updates will be effective January 1, 2026.
Do these changes apply to Remote Therapeutic Monitoring (RTM)?
Similar changes are proposed for RTM codes, including new options for shorter monitoring periods and lower time thresholds, but the specific requirements and reimbursement details may differ.
What about reimbursement rates?
CMS is using OPPS cost data to set rates, which means initial reimbursement for the new codes is expected to be similar to current rates, but future adjustments are likely as more data is collected and reviewed. Providers should watch for updates after the codes are in use.
How to Prepare for 2026
Review Your Current RPM Program: Assess which patients may now be eligible for RPM under the new 2–15 day rule.
Update Billing Practices: Train billing staff on the new codes and requirements.
Document Medical Necessity: Ensure ongoing documentation supports the need for RPM services.
Stay Informed: Submit comments to CMS if you have feedback on the proposed rule before the September 12, 2025 deadline. Federal Register – submit comments
Looking Ahead
The proposed 2026 changes to RPM codes are designed to make remote monitoring more practical, flexible, and financially sustainable for providers. By removing outdated barriers and reflecting real-world care patterns, CMS is positioning RPM as a core tool for modern, proactive healthcare.
For more information, see the official CMS proposed rule or consult with our billing and compliance experts to ensure a smooth transition to the new requirements.
If your practice is considering launching remote patient monitoring, now is the right time to get started. Our team can guide you through every step—program design, staff training, billing setup and more—so you can offer RPM confidently and compliantly. Contact us to learn how you can implement a successful digital care program that fits your workflow.
We'll email your breakdown and reach out to find a time.
Prefer to grab a time now?